Rethinking anxiety by providing an insight into its construction and deconstruction |
 |

By Sharon Hartles - December 2017
According to Angela Patmore author of 'The Truth about Stress' (2006) the concept of anxiety as it can be understood in today's terms did not exist five decades ago.
"If we go back fifty years people didn't use the word anxiety because there was no concept" (Angela Patmore, 2017).
This is not surprising because Jean Twenge, asserts that an era of anxiety can be more better understood as a twenty-first century phenomenon. The combinations of Angela Patmore's (2017) and Jean Twenge's (2000) comments indicate that there has been a process by which understandings of anxiety have been constructed.
The American Psychiatric Association (APA) through their publications of the Diagnostic and Statistical Manual of Mental Disorders (DSM) have constructed the medicalisation of anxiety. This was done through the shared standard language between clinicians, researchers, and public health officials within America and the countries within the European Union.
'Anxiety problems affect around 60 million people across Europe'(Hans-Ulrich Wittchen et al., 2011).
It can be implied from Angela Patmore's and Jean Twenge's assumptions that today's understandings of anxiety were constructed between the latter part of the twentieth century and the early part of the twenty-first century.
'The second half of the twentieth century saw the medicalisation of what were previously thought of as normal human experiences of worry'(Peter Conrad, 1992).
This coincides with the publication of DSM-III in which the construction of anxiety as a diagnostic category first appeared in 1980. At which stage anxiety neurosis was split into two distinct categories these being: generalized anxiety disorder (GAD) and panic disorder. In 2013, the DSM-5 was published and in contrast to the 1980's publication, the revised version has twelve constructed categories of anxiety disorders.
'In the United States, up to 18 per cent of people meet the criteria for anxiety disorders' (Ronald C Kessler et al., 2005).
Although the Diagnostic and Statistical Manual of Mental Disorders (DSM-5) was published in 2013, multi-field studies were conducted from the beginning of 2000, meaning that the DSM-5 took over a decade to develop. The method of multi-field studies, this being real world trials, enabled clinicians to diagnose and label patients with the APA's newly constructed categories of anxiety.
Data collected through a web-based research method via an electronic data capture system, from patients and clinicians, provided feedback to the DSM-5 Task Force on the dispersal of their constructed categories of anxiety. This is how the medicalisation of the APA's concept of anxiety was circulated into societies through shared discourse between professionals and lay people.
'The DSM introduced the explicit diagnostic criteria of mental disorders. This effort was aided by extensive work on constructing and validating the diagnostic criteria'(Psychiatry.org, 2017).
Richard Eckersley author of 'Is modern Western culture a health hazard?' (2005) produced evidence concerning the role culture plays in the construction of anxiety. He asserts that culture is underestimated because it is overlooked in favour of a host of other influences. The ways anxiety is understood, experienced and medicalised is culturally specific. Within Western cultures, regardless of gender, class, and ethnicity, anxiety is experienced through the same shared understandings, these being those that were constructed by the APA.
'Anxiety is a more commonly reported experience in Western countries. Prevalence is reported as high as 18 per cent in the United States, around 13 per cent in Europe, and as low as 2–4 per cent in East Asian countries'(Laura McGrath, 2017).
Modern Western cultures have constructed, categorised and medicalised anxiety. Potential causes of anxiety can be linked to inequality, individualism and materialism. In other words anxiety can be associated with a whole host of everyday experiences and social interactions.
'The medicalisation of anxiety is ‘a process whereby more and more of everyday life has come under medical domination, influence and supervision’(Irving Kenneth Zola, 1983).
Richard Eckersley drew upon a range of other researchers qualitative (rich and in-depth) and quantitative (numerical and statistical) data and exercised a multidisciplinary synthesis method to demonstrate why the construction of anxiety is not experienced or medicalised in the same way across cultures.
Richard Eckersley makes effective use of Pierre Felix Bourdieu's concept of habitus and Archana Singh-Manoux and Michael Marmot's notion of socialization to support his claims. From birth, an individual's innate thoughts and feelings become intertwined and shaped by the habitus. How one should feel, behave, react and cope to any given event or situation is embedded through cultural and social norms.
Through socialisation, attitudes, beliefs, and behaviours are shared between generations. Within Western cultures if an individual has difficulty in dealing with problems, which occur within normal everyday life routines, for example if their innate feelings, thoughts, reactions and behaviours override their socialised feelings of how they should respond, these are recognised as demonstrating the symptoms relating to anxiety. This is because APA's constructed understandings of what feelings, thoughts, reactions and behaviours constitute anxiety has also been socialised into Western cultures and are accepted as taken for granted understandings.
"The construction of anxiety has medicalised lots and lots of different things that are perfectly normal including a lot of emotions"(Angela Patmore, 2017.)
In understanding that one's feelings and thoughts are not deemed to be, the socially accepted norm, can exacerbate them creating a negative spiralling process. Labelling an individual with anxiety can reproduce anxiety, until this becomes the natural response, which then becomes a habit.
Cognitive Behavioural Therapy (CBT) examines thoughts, behaviours and daily routines. CBT looks at changing negative belief habits into positive belief habits.
A key approach in CBT is what is known as the ‘ABC’ method.
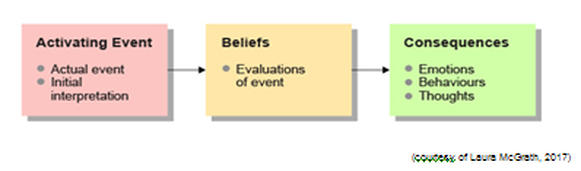
The ABC method focuses on thoughts and feelings what shape experiences and behaviours, and not the events. It deconstructs the cognitive distortions or cognitive errors negative mindset, which has been ingrained through habits, for example that one's feelings are not those which are considered to be the accepted cultural norm, but are those recognised under APA's medicalised construction of anxiety.
A positive belief mindset can deconstruct one's existing negative habits. CBT can take months or even years to deconstruct habits, which have been embedded through habitus and socialisation, that have became normalised throughout one's lifetime.
Useful contact:
'British Association for Behavioural and Cognitive Psychotherapies (BABCP) tel: 0161 705 4304 web: babcp.com Provides details of accredited cognitive behavioural therapy (CBT) therapists'.
(Courtesy of Mind, 2017 )
The Mind website also has lots of information about the different treatments that are available.
List of references
American Psychiatric Association (2017) 'DSM History' [Online] Available at
https://www.psychiatry.org/psychiatrists/practice/dsm/history-of-the-dsm (Accessed 7 December 2017)
Conrad, P (1992) ‘Medicalization and social control’, Annual Review of Sociology, vol. 18, no.1, pp. 209-232.
Kessler, R. C., Berglund, P., Demler, O., Jin, R., Merikangas, K. R. and Walters, E. E. (2005) ‘Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication’, Archives of General Psychiatry, vol. 62, no. 6, pp. 593–602
Patmore, A. (2017) 'Stress', The Davina Hour (S1 E7) [Online]. Available at
https://w.uktv.co.uk/shows/the-davina-hour/episodes/ (Accessed 9 December 2017)
Wittchen, H. U., Jacobi, F., Rehm, J., Gustavsson, A., Svensson, M. and Jonsson, B., (2011) ‘The size and burden of mental disorders and other disorders of the brain in Europe 2010’, European Neuropsychopharmacology vol. 21, pp. 655–679
Zola, I, K., (1983) 'Socio-Medical Inquiries' Wiley Online Library (2008) [Online]. Available at http://onlinelibrary.wiley.com/doi/10.1111/1467-9566.ep10831558/pdf (Accessed 9 December 2017).
ont-family:"Tahoma","sans-serif"'>(Accessed 7 December 2017)
A positive belief mindset can deconstruct one's existing negative habits. CBT can take months or even years to deconstruct habits, which have been embedded through habitus and socialisation, that have became normalised throughout one's lifetime.
Useful contact:
'British Association for Behavioural and Cognitive Psychotherapies (BABCP) tel: 0161 705 4304 web: babcp.com Provides details of accredited cognitive behavioural therapy (CBT) therapists'.
(Courtesy of Mind, 2017 )
The Mind website also has lots of information about the different treatments that are available.
List of references
American Psychiatric Association (2017) 'DSM History' [Online] Available at
https://www.psychiatry.org/psychiatrists/practice/dsm/history-of-the-dsm (Accessed 7 December 2017)
Conrad, P (1992) ‘Medicalization and social control’, Annual Review of Sociology, vol. 18, no.1, pp. 209-232.
Kessler, R. C., Berglund, P., Demler, O., Jin, R., Merikangas, K. R. and Walters, E. E. (2005) ‘Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication’, Archives of General Psychiatry, vol. 62, no. 6, pp. 593–602
Patmore, A. (2017) 'Stress', The Davina Hour (S1 E7) [Online]. Available at
https://w.uktv.co.uk/shows/the-davina-hour/episodes/ (Accessed 9 December 2017)
Wittchen, H. U., Jacobi, F., Rehm, J., Gustavsson, A., Svensson, M. and Jonsson, B., (2011) ‘The size and burden of mental disorders and other disorders of the brain in Europe 2010’, European Neuropsychopharmacology vol. 21, pp. 655–679
Zola, I, K., (1983) 'Socio-Medical Inquiries' Wiley Online Library (2008) [Online]. Available at http://onlinelibrary.wiley.com/doi/10.1111/1467-9566.ep10831558/pdf (Accessed 9 December 2017).
ont-family:"Tahoma","sans-serif"'>(Accessed 7 December 2017)
